
How to Prevent Patient Falls: Safe Solutions for 2026
📋 KEY TAKEAWAYS
Updated June 2026: This article was previously published at an earlier date and has been updated with new product information and 2026 recommendations.
-
-
Assess fall risk first. Identify whether the risk comes from medications, vision, footwear, the environment, the bed, or the transfer, because the fix depends on the cause.
-
Modify the environment. Remove loose rugs, improve lighting, add grab bars in bathrooms, and ensure bed height allows safe standing without strain.
-
Use the right equipment. A mobility aid for walking, a fall mat beside the bed, and an ultra-low hospital bed for high-risk patients each address a different moment of fall risk.
-
Train every caregiver involved. Safe transfer technique, medication timing awareness, and consistent risk communication at every handoff are as important as any piece of equipment.
- Falls are the leading cause of injury-related death among older adults, and most are preventable with the right combination of environment, equipment, and care habits.
- No single fix prevents all falls. The most effective approach addresses medication risks, vision, footwear, environment, bed safety, transfers, and caregiver training together.
- Products and beds are only one part of the solution. This guide covers the full picture so caregivers and home health providers can act on every layer of fall risk.
- Browse High Low Hospital Beds designed specifically for fall prevention at home and in long-term care.
Top Equipment:- Medacure Steel Rollator: Best Mobility Aid
- Proactive Medical Protekt Beveled Fall Mat: Best Bedside Fall Buffer
- Medacure ULB 3.9: Best Ultra-Low Bed
- Independence Rotating Bed: Best for Safe Sit-to-Stand Transfers
Bottom Line: Falls don't happen for one reason and they don't get prevented by one fix. The caregivers who reduce fall rates most are the ones who address the whole picture.
-
Assess fall risk first. Identify whether the risk comes from medications, vision, footwear, the environment, the bed, or the transfer, because the fix depends on the cause.
Understanding Why Patients Fall
Patient falls are one of the most serious challenges in home care and healthcare facilities, with up to one million patients falling each year in U.S. hospitals alone. Falls result from a combination of factors working together, not a single cause.
Understanding those causes is the starting point for any effective prevention strategy.
4 Intrinsic Risk Factors That Increase Fall Risk

These are patient-related factors that caregivers need to assess individually:
- Age-related physical changes, Older adults experience declining muscle strength, slower reflexes, and reduced balance. These changes are gradual and easy to underestimate until a fall occurs.
- Chronic conditions, Parkinson's disease, arthritis, stroke, and neurological disorders all affect physical stability and movement control.
- Cognitive impairment, Patients with dementia or Alzheimer's may not recognize environmental hazards or understand their own physical limitations. They are among the highest-risk individuals for nighttime falls.
- Medication side effects, Sedatives, antidepressants, blood pressure medications, and diuretics can all cause dizziness, reduced coordination, or sudden blood pressure drops that lead to falls.
According to the National Institute on Aging, more than one in four adults aged 65 and older fall each year. Identifying which intrinsic factors apply to a specific patient shapes every other prevention decision.
Environmental and Systemic Fall Hazards
The environment surrounding a patient contributes as much to fall risk as the patient's own condition. The AHRQ patient safety resources identify the following as consistent environmental contributors:
- Poor or inadequate lighting in hallways, bathrooms, and bedrooms
- Cluttered walkways and unsecured floor rugs
- Slippery surfaces without grip strips or non-slip mats
- Beds and chairs at heights that make standing difficult
- No grab bars in bathrooms or near the toilet
Systemic issues inside care facilities add another layer. Insufficient staff communication, gaps in handoff documentation, and inconsistent fall risk assessment protocols all create conditions where high-risk patients go unprotected.
Comprehensive Fall Risk Assessment
Effective prevention requires a structured assessment that covers all risk dimensions at once. The CDC STEADI program (Stopping Elderly Accidents, Deaths, and Injuries) provides a widely used clinical framework for screening older adults, identifying risk factors, and selecting targeted interventions.
A complete assessment should address physical capability, cognitive status, medication list, fall history, environmental conditions, and footwear. It should be repeated whenever a patient's condition or care setting changes, not just on admission.
Medication-Related Fall Risks
Medications are among the most underestimated fall contributors, yet they are also among the most actionable. When a patient is on four or more medications, fall risk increases significantly.
The highest-risk drug categories include:
- Sedatives and sleep aids, cause residual drowsiness and impaired balance
- Blood pressure medications, can cause orthostatic hypotension, the sudden drop in blood pressure that occurs when standing
- Diuretics, increase nighttime bathroom trips, when falls are most common
- Antidepressants, affect coordination and reaction time
- Antihistamines, cause sedation, especially in older adults
Caregivers should review medication lists with a physician or pharmacist at every care transition. Timing adjustments, such as giving diuretics earlier in the day, can reduce nighttime movement without changing the treatment itself.
Vision and Footwear: Two Overlooked Fall Triggers
Vision
Uncorrected vision problems reduce a person's ability to detect floor hazards, judge distances, and navigate in low light. Many older adults go months or years between eye exams, and even those wearing glasses may be using an outdated prescription.
Bifocals are a specific hazard on stairs and uneven surfaces. The distortion at the lower portion of a bifocal lens affects depth perception precisely in the situations where accurate judgment matters most.
Annual vision screening is a basic fall prevention step that is frequently missed.
Footwear
Non-slip soles are not optional for fall-risk individuals. Loose slippers, socks on hard floors, and worn shoes with smooth soles are each a fall setup on their own.
Footwear should fit securely, have a low heel, and provide grip on all indoor surfaces. This is one of the simplest and least expensive fall prevention interventions available, and one of the most consistently ignored.
Environmental Hazards and Home Safety
Home environments contain hazards that become invisible through familiarity. A caregiver who has walked past the same loose rug for two years may not see it as a risk. A patient who fell last month may have fallen on that same rug.
A structured walkthrough should cover:
- Bedroom: Clear path from bed to bathroom, nightlight or motion-sensor lighting, bed at correct height for safe standing
- Bathroom: Grab bars next to toilet and in shower, non-slip mat in tub, raised toilet seat if needed
- Hallways and stairs: Adequate lighting, handrails on both sides of stairs, no cords crossing pathways
- Living areas: Furniture positioned to create stable support surfaces, chairs and sofas at heights that allow safe standing
Environmental modifications are low-cost and high-impact. Many can be implemented in a single afternoon.
Transfer Assistance and Safe Bed Exits
The moments of getting in and out of bed carry the highest fall risk in any care environment. Most nighttime falls happen during an unassisted transfer attempt.
Two things can be done to address this. The first is reducing what happens if a fall occurs. The second is making the transfer itself safer.
Reducing fall consequences means lowering the bed surface as close to the floor as possible. A mattress at 3.9 inches from the floor involves almost no meaningful fall distance. Hospital beds with genuine ultra-low positioning address this directly.
Reducing transfer risk means giving the patient mechanical assistance through the sit-to-stand movement. Specialized rotating beds eliminate the dangerous sideways pivot by bringing the patient to face their caregiver or walking aid before standing begins.
Safe transfer technique for all caregivers includes:
| Step | Description | Purpose |
|---|---|---|
| Assess patient capabilities | Evaluate strength, balance, cognition, and mobility | Choose the safest transfer method |
| Explain the transfer process | Communicate step-by-step instructions to the patient | Increase confidence, reduce anxiety |
| Move slowly and deliberately | Patient instructed to move carefully, not rush | Prevent dizziness, ensure controlled movement |
| Sit at bed edge | Patient sits and pauses before standing | Allow blood pressure to stabilize, reduce dizziness |
| Pause before standing | Encourage patient to pause after position changes | Prevent sudden balance loss |
| Use transfer aids if needed | Employ gait belts or transfer boards as appropriate | Provide support, reduce physical strain |
| Caregiver support | Caregiver provides hands-on physical and verbal guidance | Coordinate movement, offer security |
One specific technique for patients with limited mobility is the log roll method: guide the patient to roll onto their side, use their arms to push into a sitting position, then pause at the edge before standing with caregiver support. Gait belts provide additional security during these movements, allowing the caregiver to offer physical guidance without strain on either person.
The WHO fall prevention resources note that falls are the second leading cause of accidental injury deaths worldwide, with older adults carrying the greatest burden. Safe transfer practice is one of the most consistently effective interventions across care settings.
Mobility Aids for Fall Prevention
Mobility aids reduce fall risk during walking. They are not a concession to dependence, they are prevention tools. A patient who refuses a walker and falls carries far greater risk than one using a rollator with confidence.
Rollators are four-wheeled walkers with hand brakes and a built-in seat. They provide stability during walking and a rest surface when fatigue sets in, because fatigue during walking is itself a fall risk.
Standard walkers offer maximum base support for patients with significant weakness or balance deficits.
Canes provide lighter support for patients with minor imbalance who still have reasonable strength.
The right aid matches the patient's actual support needs and the surfaces they navigate daily.
Medacure Steel Rollator, 6" Wheels for Indoor and Outdoor Use
The Medacure Steel Rollator provides dependable support for safer mobility both indoors and outdoors. The 6" casters roll smoothly over thresholds, uneven flooring, and outdoor surfaces that smaller-wheeled alternatives catch on. Dual hand grip brakes provide maximum control, including when stopping on a slope.
The ergonomic handles adjust from 29.5" to 38" to fit different user heights. The padded seat (13"W x 12"D, 18"-22" from floor) provides a stable rest surface during longer distances. The storage basket carries daily essentials so the patient's hands stay on the handles.

Key Specs, Medacure Steel Rollator
- Handle Height Range: 29.5" to 38"
- Seat Height: 18" to 22"
- Seat Width: 13" / Seat Depth: 12"
- Inside Hand Grip Width: 17"
- Weight Capacity: 300 lbs
- Casters: 6" x 4
- Material: Steel
- Dimensions: 24"W x 27"L
- Product Weight: 14 lbs
- Colors: Black, Red, Blue
GET THIS IF your patient is mobile but needs stability support during walking, especially for longer distances or mixed indoor and outdoor environments.
See Product
Safety Equipment for Patient Environments
Beyond mobility aids, certain bedside and bathroom equipment addresses the physical environment directly.
Grab bars near the toilet and in the shower provide fixed support points that furniture cannot reliably substitute for. They should be anchored to wall studs, not just drywall.
Raised toilet seats reduce the effort required for sitting and standing, lowering the strain on legs and core that can cause loss of balance during bathroom use.
Non-slip mats in bathrooms and on hard floors provide grip where smooth surfaces would otherwise create slide risk.
Bed exit alarms alert caregivers when a high-risk patient attempts to leave the bed unassisted, allowing intervention before a fall occurs.
The table below summarizes essential fall prevention equipment by category:
| Type of Equipment | Examples | Primary Purpose |
|---|---|---|
| Mobility Devices | Walkers, Canes, Rollators | Provide stability during walking and movement |
| Transfer Aids | Gait Belts, Transfer Boards | Assist with safe patient transfers between surfaces |
| Environmental Safety | Bed Exit Alarms, Non-slip Mats | Alert staff and reduce risk in patient environments |
| Bathroom Safety | Grab Bars, Raised Toilet Seats | Support safe bathroom use |
| Bedside Protection | Fall Mats | Cushion accidental roll-outs from bed |
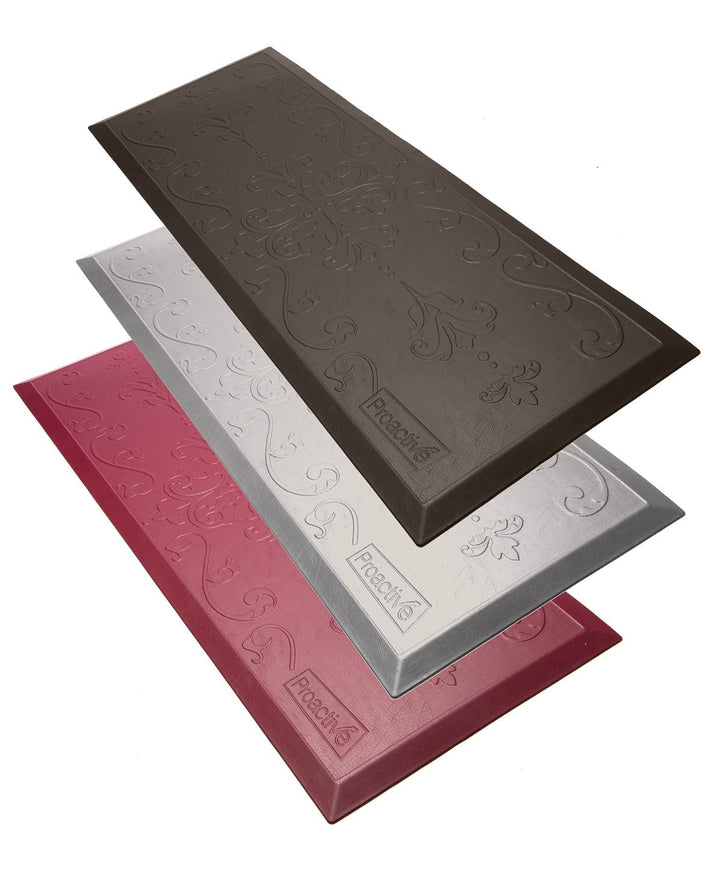
Proactive Medical Protekt Beveled Fall Mat, Thinnest Profile Available
The Protekt Beveled Fall Mat cushions falls from bed, reducing injury risk from accidental roll-outs. At under 0.7 inches, it is the thinnest fall mat available, low enough that wheelchairs and lifts can pass over it without resistance, and beveled edges prevent the mat's own border from becoming a tripping hazard.
The vinyl polymer material is impact-resistant, anti-microbial, anti-bacterial, and wipes clean with standard cleaning solutions. The non-skid bottom keeps the mat in position during movement around the bed. Anti-fatigue properties also provide extra comfort for caregivers standing beside the bed during care tasks.
Key Specs, Proactive Medical Protekt Beveled Fall Mat
- Dimensions: 70"L x 24"W x 0.7"H
- Profile: Under 0.7", thinnest available
- Material: Vinyl polymer, impact-resistant, anti-microbial, anti-bacterial
- Bottom: Non-skid
- Edges: Beveled for wheelchair and lift pass-over
- Colors: Brown, Grey, Maroon
GET THIS IF a patient is at risk for nighttime bed roll-outs, or is in a bed that cannot be lowered close to floor level, this mat provides the last line of impact cushioning if a fall occurs.
See Product
How Hospital Bed Design Can Help Reduce Fall Risk
Hospital bed design is a direct fall prevention variable. The two features that matter most are low-end height range and hi-low adjustability.
Low-end height range determines how close the mattress surface gets to the floor. The difference between a bed at 15 inches and a bed at 3.9 inches is the difference between a serious injury risk and almost none if a patient rolls out.
Hi-low adjustability serves two groups simultaneously. At the low end, it protects patients by reducing fall distance. At the high end, it raises the surface to a comfortable working height for caregivers, eliminating the repeated bending that causes back injury over time.
A bed without a wide enough height range cannot serve either function fully. Range matters more than the existence of the feature.
Medacure ULB 3.9, Lowest Electric Hospital Bed on the Market
The Medacure ULB 3.9 descends to 3.9 inches from the floor, the lowest electric hospital bed available. It is designed specifically for fall prevention in seniors with dementia, Alzheimer's, or any condition that creates uncontrolled nighttime bed exit risk.
At 3.9 inches, the sleeping surface is near floor level. When a patient attempts to exit the bed at night, the fall distance is minimal. During the day, the bed raises to 25 inches, a comfortable height for caregiving, medication administration, and personal hygiene without back strain.
The 10-function hand pendant controls Hi/Lo, Head, Foot, Trendelenburg, Reverse Trendelenburg, and Auto Contour. Premium LINAK actuators provide quiet, reliable operation. The split frame design folds to 36"L x 20"W x 48.5"H for transport through standard residential doorways or storage when not in use.

Key Specs, Medacure ULB 3.9
- Height Range: 3.9" to 25"
- Functions: 10-function electric: Hi/Lo, Head, Foot, Trendelenburg, Reverse Trendelenburg, Auto Contour
- Weight Capacity: 450 lbs
- Mattress Deck: 36"x80" (42" bariatric option available)
- Actuators: LINAK
- Castors: 4 x 3" locking casters
- Split Frame Folded Dimensions: 36"L x 20"W x 48.5"H
- Includes: Two patient assist bars, mattress retainers on all four corners
- Mattress Options: Not listed
- Warranty: Not listed
GET THIS IF your patient has dementia, Alzheimer's, or a history of nighttime bed exits, the 3.9-inch low position is the most effective bed-based fall prevention available.
See Product
Independence Rotating Bed, For Safe Sit-to-Stand Transfers
For many patients, the fall does not happen from the bed. It happens during the attempt to stand. A flat mattress requires a sideways pivot with no mechanical support, a movement that frequently causes loss of balance before the patient's feet are properly under them.
The Independence Rotating Bed addresses the transfer itself. The entire platform rotates 90 degrees, bringing the patient to face their walker, wheelchair, or caregiver before standing begins. A Lift Assist position gently tilts the patient forward to help initiate standing, reducing the physical effort required and the risk that comes with it.
The bed includes a 6" premium memory foam mattress (3" gel-infused cooling layer plus 3" high-density support foam), underbed safety lighting, dual USB ports on both sides, removable side arms, an emergency battery backup, and a hard-wired remote with handrail clip. White glove delivery and setup are included.
Note: the Independence Bed tilts, the platform does not raise and lower in the standard hi-low sense.

Key Specs, Independence Rotating Bed
- Rotation: 90 degrees, left or right configurable
- Twin XL: 38"W x 80"L, 25"H to mattress surface, 33"H to top of handrail, 316 lbs assembled
- Twin: 38"W x 75"L, 23"H to mattress surface, 31"H to top of handrail, 270 lbs assembled
- Weight Capacity: 500 lbs (both sizes)
- Mattress: 6" premium memory foam included (3" gel cooling + 3" support foam)
- Features: Underbed safety lighting, dual USB ports both sides, removable side arms, emergency battery backup, hard-wired remote with handrail clip
- Warranty: 10-year limited (Year 1: parts and labor; Years 2-3: parts only; Years 4-10: frame and non-electric mechanisms)
- Delivery: White glove delivery and setup included
GET THIS IF your patient falls during the transfer out of bed rather than from the bed itself, the rotation and lift-assist function address the transfer movement directly.
See Product
Staff and Caregiver Education
Equipment and environment address a large portion of fall risk. Caregiver knowledge and consistency address the rest.
Key education areas include:
- Fall risk communication, clearly flagging high-risk patients at every shift change and care handoff
- Safe transfer technique, proper body mechanics that protect both patient and caregiver
- Medication awareness, knowing which medications in a patient's current regimen increase fall risk
- Environmental rounds, building regular safety checks into daily care routines
- Post-fall documentation and review, treating every fall as data for improving the care plan
Caregiver education is not a one-time training. Fall prevention knowledge needs to be reinforced as patient conditions change, as staffing changes, and as care environments evolve.
Recommended products for fall prevention:
- Medacure ULB 3.9
- Proactive Medical Protekt Beveled Fall Mat
- Medacure Steel Rollator
- Independence Rotating Bed
Frequently Asked Questions
How do you prevent patient falls at home? Use a layered approach: review medications, address vision and footwear, fix environmental hazards, use a mobility aid, and choose a bed with genuine hi-low functionality.
What is the most effective fall prevention tool for elderly patients? No single tool covers all risk. For bed-based fall prevention, the Medacure ULB 3.9 at 3.9 inches is the lowest-profile option available. Pair it with a bedside fall mat for maximum protection.
What are fall prevention strategies in home care environments? Structured risk assessment, medication review, environmental modifications, correct footwear, mobility aids, safe transfer training, and appropriate bed height adjustment.
What is the CDC STEADI program? STEADI stands for Stopping Elderly Accidents, Deaths, and Injuries. It is a CDC initiative providing healthcare providers with screening tools, risk assessment frameworks, and intervention guides for older adult fall prevention.
When should a rollator be used instead of a standard walker? When a patient needs stability during walking but also needs the ability to rest during longer distances. The built-in seat and hand brakes of a rollator make it safer than a standard walker for patients who fatigue easily.
How does bed height affect fall risk? The lower the bed, the shorter the fall distance if a patient rolls out or exits uncontrolled. A mattress at 3.9 inches from the floor involves almost no meaningful fall distance. A standard bed at 16 to 20 inches carries a significant injury risk for the same event.
What is the difference between a fall mat and a non-slip mat? A fall mat is placed bedside to cushion impact from a roll-out. A non-slip mat prevents slipping on hard floors, typically in bathrooms or kitchens. Both serve different purposes and are often used together in high-risk environments.
Featured collection


$3,444.77
-
$6,889.54
$3,444.77
-
$6,889.54
Current price
$3,444.77
Original price
$3,444.77
-
Original price
$6,889.54
Original price
Luxury Electric Hospital Bed - Hospital Functions Without the Hospital Look | TransferMaster Supernal 3
TransferMaster
In stock
Ships Next Day
$3,444.77
-
$6,889.54
$3,444.77
-
$6,889.54
Current price
$3,444.77
Original price
$3,444.77
-
Original price
$6,889.54
Original price
$3,444.77
-
$6,889.54
$3,444.77
-
$6,889.54
Current price
$3,444.77
Original price
$3,444.77
-
Original price
$6,889.54
Original price


$4,250.00
-
$7,450.00
$4,250.00
-
$7,450.00
Current price
$4,250.00
Original price
$4,250.00
-
Original price
$7,450.00
Original price
Adjustable Homecare Hospital Bed – iCare IC333 Medical Bed
Icare
In stock
Ships Next Day
$4,250.00
-
$7,450.00
$4,250.00
-
$7,450.00
Current price
$4,250.00
Original price
$4,250.00
-
Original price
$7,450.00
Original price
$4,250.00
-
$7,450.00
$4,250.00
-
$7,450.00
Current price
$4,250.00
Original price
$4,250.00
-
Original price
$7,450.00
Original price


Current price
$3,599.00
$3,599.00
-
$3,599.00
Current price
$3,599.00
Original price
$4,999.99
Original price
$4,999.99
-
Original price
$4,999.99
Original price
$4,999.99
Adjustable Rotating Bed for Seniors | Sit to Stand Lift Bed | Independence Bed
Customatic
Only 3 left!
Ships Next Day
Current price
$3,599.00
$3,599.00
-
$3,599.00
Current price
$3,599.00
Original price
$4,999.99
Original price
$4,999.99
-
Original price
$4,999.99
Original price
$4,999.99
Current price
$3,599.00
$3,599.00
-
$3,599.00
Current price
$3,599.00
Original price
$4,999.99
Original price
$4,999.99
-
Original price
$4,999.99
Original price
$4,999.99
You save $1,400.99 (28%)


Current price
$2,460.83
$2,460.83
-
$2,460.83
Current price
$2,460.83
Original price
$2,934.00
Original price
$2,934.00
-
Original price
$2,934.00
Original price
$2,934.00
Full Electric Bariatric Bed - Hi Low Hospital Bed 650 LB Capacity | Emerald Infinity 54000
Emerald
Only 1 left!
Ships Next Day
Current price
$2,460.83
$2,460.83
-
$2,460.83
Current price
$2,460.83
Original price
$2,934.00
Original price
$2,934.00
-
Original price
$2,934.00
Original price
$2,934.00
Current price
$2,460.83
$2,460.83
-
$2,460.83
Current price
$2,460.83
Original price
$2,934.00
Original price
$2,934.00
-
Original price
$2,934.00
Original price
$2,934.00
You save $473.17 (16%)


Current price
$2,290.00
$2,290.00
-
$2,290.00
Current price
$2,290.00
Original price
$2,499.00
Original price
$2,499.00
-
Original price
$2,499.00
Original price
$2,499.00
High Low Electric Hospital Bed with Rails for Fall Prevention | 36" x 80" | Medacure ULB 3.9
Medacure
In stock
Ships Next Day
Current price
$2,290.00
$2,290.00
-
$2,290.00
Current price
$2,290.00
Original price
$2,499.00
Original price
$2,499.00
-
Original price
$2,499.00
Original price
$2,499.00
Current price
$2,290.00
$2,290.00
-
$2,290.00
Current price
$2,290.00
Original price
$2,499.00
Original price
$2,499.00
-
Original price
$2,499.00
Original price
$2,499.00
You save $209.00 (8%)